


Your Favorite Transgender Activists Used "Hard" Drugs, Sold Sex, and Pioneered Harm Reduction
The dominant ways in which drug use in the LGBTQIA community is addressed is weirdly reactionary and it's unsettling

Minority stress theory, developed by Ilan H. Meyer, posits that minority groups experience chronic stress due to their marginalized status in society. This stress can lead to negative health and mental health outcomes. Given this information, the logical thing to do to “help” marginalized communities such as the trans/gender non-conforming (TGNC) community is perpetuate drug use stigma and propaganda.
I’m obviously joking.
Sadly, many people are not—Including within the LGBTQIA+ community. I know this is not the intent, usually. However in discouraging drug use, people often fall back on anti-drug/drug war style propaganda, which further creates shame, guilt, and isolation. This is extremely harmful to our community, as queer folks have the highest rates of drug use, and it’s estimated that trans women have the highest rates of drug use out of them all. An estimated 20 to 30% of the LGBTQ+ community uses substances, compared to about 9% of the general population. We need to get real about harm reduction, and I’m really talking to my own community with this one since apparently many have learned nothing from queer elders and movement workers of the 80s and 90s (not all of them are dead, either).

Minority stress theories suggest that high rates of discrimination experienced by transgender people are precipitants of substance use. This risk is exacerbated by an inadequate provision of trans-inclusive substance use services, as well as the fact that we have hardly any data around trans folks that use drugs.
Minority stressors include, but are not limited to:
Discrimination in employment, education, or healthcare
Microaggressions and subtle forms of prejudice
Experiences of violence or harassment
Lack of cultural representation and acceptance
Chronic minority stress can have a significant impact on health, including:
Increased risk of cardiovascular disease, stroke, and diabetes
Higher rates of mental health disorders, such as depression and anxiety
Lower life expectancy
Weakened immune system
Minority stress theory highlights the importance of addressing the social and structural factors that contribute to marginalization and its negative health consequences.
Sometimes it’s our own community, “allies” piling on additional stress

She’s probably right that there are loads of “new young queers” on the scene getting into drugs, but let’s consider this important context: Studies suggest Gen Z-ers drink less alcohol, however, as rates of drinking are decreasing, drug use is on the rise. Gen Z drug use outpaces all other age groups for factors such as [recreational] prescription benzodiazepine use and cocaine use. This makes harm reduction possibly more important than before. I mean REAL harm reduction—the harm reduction the LGBTs of Gen X pioneered. Not this half-baked “only do drugs we think are ‘soft’” messaging based on no supporting evidence, just anecdotes, or only supporting harm reduction as a pathway to mandatory sobriety/abstinence.

Harm reduction meets people where they’re at.
In Vietnam, 20% of all American troops were using heroin en masse, and the public was worried that there would be “hundreds of thousands of junkies on the streets” when the war ends; The Archives of General Psychiatry did a detailed study on these heroin-using soldiers, and it turns out they didn't go to rehab and they didn't go into withdrawal. 95% of them just stopped.
I you believe addiction is only about chemical hooks, then this phenomenon makes absolutely no sense. We’ve heard of Rat Park, by now, right? We’ve had this research for DECADES, yet for some reason society holds onto sensationalist narratives and fear mongering. More-so than chemical hooks, addiction is an adaptation to your environment.
“… And you know, because of the lifestyle most of us had, you had to get involved with drugs. Because you had to be out when a time when most people are sleeping. And you have to be out during the day because you can’t be where you are at night safely to sleep. And so, having to go through all of that, you have to have something to keep you going. And so a lot of the girls were either doing drugs or drinking, you know. And the community around, always berated it/us for doing that and how horrible we were and that made us addicts and junkies. No we were people that needed this shit to survive. We weren’t doing this shit for fun. It wasn’t something we did because “oh girl I don’t know what to do today, oh I’ll just shoot :’ drugs”. And so through that premise about us they berated us and read us a lot. Especially those white fags down there. Those little arrogant chauvinist ass, preppy ass, white privilege mother fuckers gave us a whole bunch of shit on a regular basis. Which they still do. So.” — Miss Major Griffin-Gracy, a community organizer that drove San Francisco’s first needle exchange van during the AIDS epidemic

Community needs solidarity building. It’s not defined by like aesthetics, groupthink, and cliques.
Isolation is something I’ve spoken about a number of times, primarily to the psychedelics/natural “medicine” community. Medicine in quotations, because I think most of the community is full of shit. They are 21st century cultists selling people on the idea that specific substances will fix your life without attempting to address a single root cause of mental illness or behavioral disorders. I recently referred to this as “white people trying to medicate away white people’s problems”, and I should add “with indigenous medicines and rituals”.
They weren’t doing drugs, they were doing things to enlighten their mind... Yeah okay, take your mind, get on your knees and suck the dick like the rest of us and quit fucking bullshitting us. — Miss Major Griffin-Gracy
Speaking on the topic of community being harm reduction at MAPS Psychedelic Science 2023 (Denver) and Queering Psychedelics 2023 (San Francisco). Bonus: watch till the end to see me cry.
At this point, the “wellness” industry is substantially more profitable than “big pharma”. People will say anything to sell you on their specific “cure” or treatment. People have gone as far as lying about living with cancer to sell folks on alternative medicine. The global pharmaceutical market was estimated at around $1.6 trillion in 2023, and the global wellness industry is estimated to be worth approximately $6.3 trillion—the largest market being the United States with an estimated value of $1.8 trillion value. Let that sink in.
For the topic at hand, I’m going to pull out a handful of statistics from the 2022 U.S. Transgender Survey, since some new data has been released since the previous Trans Survey, which was published in 2015 (well before the COVID-19 pandemic and the latest series of aggressive civil rights and liberties attacks on transgender people), as well as pull up 2024 data from NEXT Distro’s TGNC participants. Since it is a LOT of information, I am creating a separate datasheet that will have all the data I’m referencing for my next few points:
Transgender Day of Visibility Factsheet 2025

Each year on March 31st, the world observes Transgender Day of Visibility (TDOV) to raise awareness about transgender people. It is a day to celebrate the lives and contributions of trans people, while also drawing attention to the poverty, discrimination, and violence the transgender and gender-nonconforming (TGNC) community faces. We recognize that ge…
What are other challenges pushing TGNC people who use drugs (PWUD) further into the margins?
If you haven’t explicitly considered how your support or services accommodate TGNC individuals and their specific needs, then I guarantee you it’s not adequate.
With 61% of TGNC respondents stating that they are going out less or not at all due to the impact of COVID-19, where does the community exist for those who are remaining cautious or do not have a choice? People still use drugs, even when they’re not going out. Using alone is how people overdose and die—as they are not found in time to receive help. Cecilia Gentili, who was a supporter of harm reduction herself passed away from an overdose that took place overnight while she was alone. 2 men were charged in distributing fentanyl laced heroin that led to her death… Hey folks, opioid users know their supply is fucked and typically have a tolerance to these very potent substances, but when drugs can vary in potency and ingredients, or someone is returns to using after a detox, overdoses can happen. Taking harsh, zero-tolerance stances doesn’t help PWUD.
Sidebar: There is NO heroin in the majority of the supply in New York anymore. We must move beyond messaging that assumes people aren’t aware or intending to use potent drugs/cocktails on their own accord, and that finding fentanyl, xylazine, and whatever other boogieman drugs the media sensationalizes, will discourage folks from using.
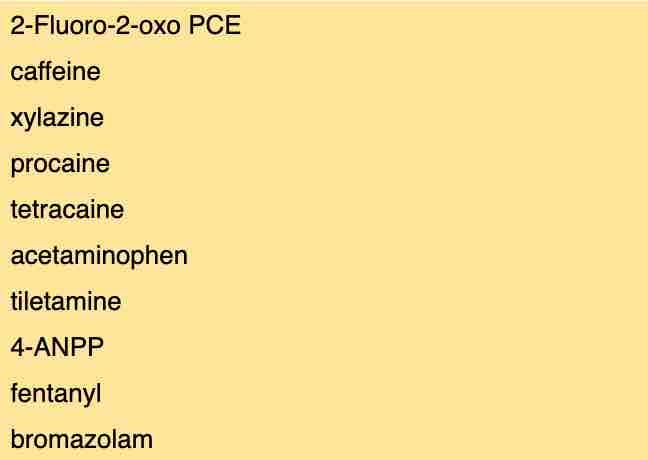
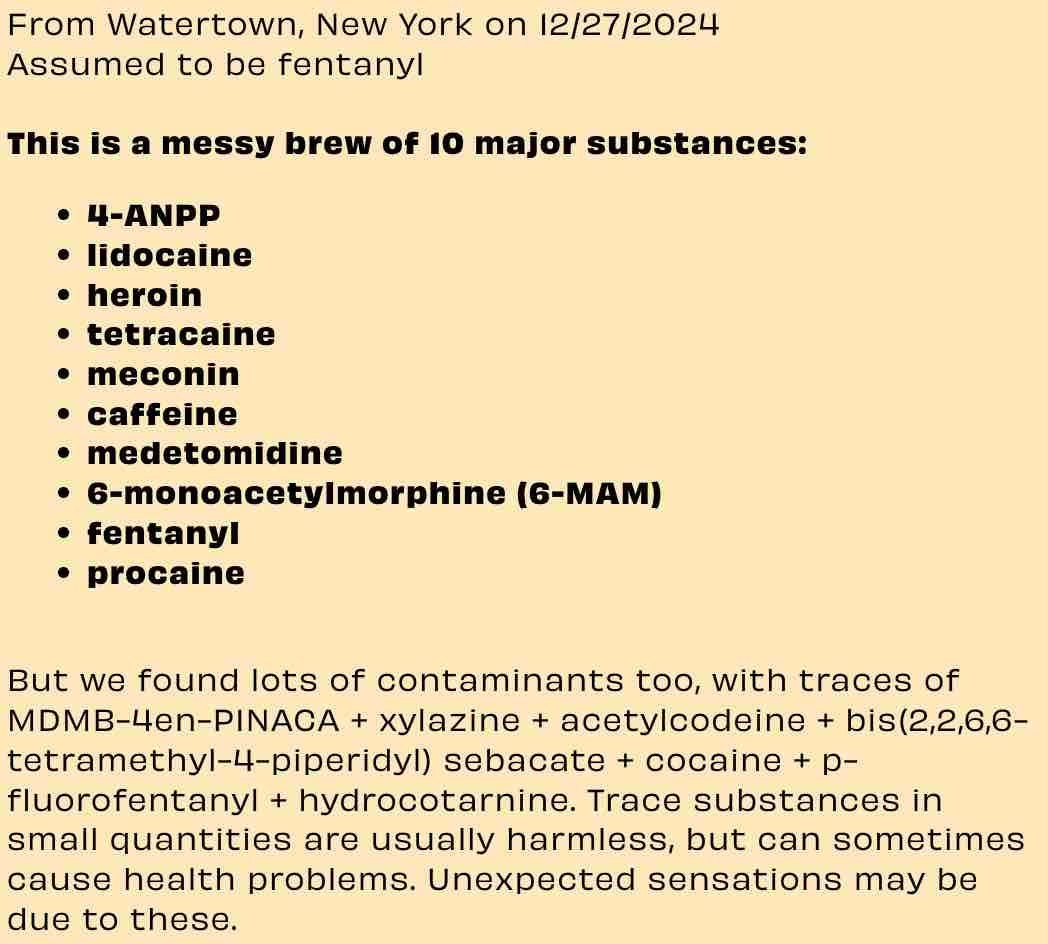
Dope usually contains fentanyl, xylazine, random other dissociative drugs like medetomidine, and the synthetic cannibinoid MDMB-4en-PINACA (rampant in the “Kush” supply in Sierra Leone, and the synthetic cannabis supply in New York). Samples that I’ve analyzed from Chicago have contained fentanyl (in 1 case carfentanil), xylazine, diphenhydramine (Benedryl), sometimes quetiapine (Seroquel), nitazenes, and maybe a sprinkle of heroin. Samples that I’ve analyzed from Ohio also contain nitazenes, xylazine, and fentanyl, although there are some sources that are fentanyl only (still no heroin to be found).
In NYC, for some reason many are still imposing a G ban at nightclubs and events—infractions of which can permanently prevent individuals from participating in these spaces. Some community members have even been banned for using G (in their personal lives), but not being caught with it on their person or under the influence of it in these spaces. I’ve been vocal against these rules for years. In 2019, I sat in a room full of venue owners and nightlife promoters at the NYC Office of Nightlife seemingly confused about what to do about G use in at their events and essentially pretended like I wasn’t even there suggesting harm reduction strategies. When working harm reduction in some of these spaces, harm reduction peers have been asked to report any G that they may encounter (usually when onsite testing is being offered). What the fuck? We’re not narcs like Bunk Police.
When I visited Amsterdam again in November of 2024, I asked their local queer nightlife harm reduction organization (Pink Unity) members what types of policies are in place in their scene, especially around drug use. Essentially, there are avenues one can take for re-entry into spaces where inappropriate conduct may have taken place. The logistics of which seem to be club specific, but basically forever removing someone from community is not something that happens. For many TGNC individuals, these 3rd spaces are the most important spaces we have for creating connections, and these connections save lives. Without them, there aren’t many other outlets available anymore for those who are staying out of public spaces—especially high occupancy/crowded spaces. Connect on social media, you say? Well, social media is a lot less productive for building deep and meaningful relationships these days. It mostly fosters confrontation and mis/disinformation spreading.
We can try to point fingers at whatever drug we want, but the bottom line is we trans folks use drugs at very high rates and fear mongering about how “dangerous” these substances are and stigmatizing users is counterproductive. These attitudes push many further into the margins.

Many folks do not understand the relative harms of drugs.
Opioids are the most treated drug in the world, but are not the most consumed. In 2009, over one million hospital visits involved an illicit drug, either alone or in combination with other types of drugs. Many of the existing interventions focus on opioid use and overdose prevention, when data shows that a large percentage of emergency department visits often involve non-opioid drugs. This data precedes the prevalence of synthetic cannabinoids and synthetic cathinones, which have also contributed to a number of medical emergencies since 2012.

Drug use is more complex than we’re perceiving—we must acknowledge polydrug use, too.
Methamphetamine, ketamine, and MDMA use has been found to be associated with increased risk for GHB use. These drugs have been the most common party drugs in the queer scene for over 2 decades, because chemsex is a thing.
Many respondents that reported that they use dissociative drugs (like Ketamine), GABA agonists (G drugs and Ambien, excluding benzos), and Benzodiazepines reported that they use alcohol. When used together, these combinations of substances can cause potentiated side effects like vomiting and severe respiratory depression.
Some respondents that reported that they take antidepressants (ADs) (SSRIs or Wellbutrin, which is an NDRI) reported that they also use sedative/dissociative drugs, stimulants, and psychedelic drugs (psychedelic drugs in the phenethylamine like MDMA, 2C-B, and 4-MMC and tryptamine classes like LSD and psilocybin modulate many of the same receptors as ADs)
Most respondents’ feedback about talking about drug use with healthcare providers state that they don't disclose any use because they know/fear there will be judgement and/or consequences. How many TGNC folks are hiding their drug use from community members who would treat them similarly? Navigating using drugs while being TGNC is a minefield.
Resources for TGNC are lacking, even with existing harm reduction services.
I asked the Director of Harm Reduction initiatives at OnPoint if TGNC folks use the space, and I was told “they used to” and that they don’t know why not very many TGNC folks utilize the space (as previous years, which still was not many). I’ll wager a guess that maybe it’s because the space feels like “the DMV mixed with a trap house”. As a harm reduction worker, I’m pretty used to working in chaotic conditions and with lots of different types of people, however, the average TGNC person is unlikely to feel comfortable in an overstimulating space and around participants and/or staff that may make them feel unsafe.1
TGNC folks are an extremely vulnerable population. Consider these important metrics
Since there aren’t specific studies on trans populations’ drug use and compounding needs, I’m using 2024 data from NEXT Distro to represent some insightful findings. I also did so in 2023.
In comparison between TGNC and non-trans people enrolled in the year 2024, the TGNC participants are:
442% more likely to have HIV
118% more likely to be BIPOC
95% more likely to be diagnosed with Cardiovascular Disease
69% more likely to have overdosed in the last year
43% more likely to have actively shared syringes with others in the last 30 days
40% more likely to be diagnosed with Hepatitis C
22% more likely to be homeless or unstably housed
5% more likely to have shared smoking supplies in the last 30 days
4% more likely to have actively reused their own syringes in the last 30 days
4% more likely to have witnessed an overdose in the last year
17% less likely to be accessing public benefits
For folks who received naloxone from the NYC office in 2024, TGNC requestors were 19% more likely than non-TGNC enrollees to not have health insurance or not know their health insurance status
In comparison between BIPOC and non-BIPOC participants enrolled in the year 2024, the BIPOC participants are 170% more likely to be TGNC.
TGNC people seek NEXT services at 26 times the rate of the US population (7.7% vs 0.3%), showing there is a significant overlap between drug users and the TGNC community. TGNC people have received services from the Distro program in 44 states and from the Naloxone program in 51 states (including DC), showing a national need for resources amongst the TGNC community.
TGNC PWUD have a significant need, and the work starts with us in our own community.

There are numerous radical TGNC harm reduction peers and advocates as this is very much a movement pioneered by the LGBTQIA community. I encourage the community to authentically connect with us, learn, and support.